- By Dr. Vinh-Kim Nguyen & Melissa C. Coyle
The world was amazed by the rapid creation of COVID-19 vaccines. In a matter of hours after learning the virus’ genetic sequence, BioNTech’s Sahin and Özlem Türeci had 10 vaccine candidates ready to experiment. The shock attributed to this accelerated development is partly because vaccine creation is a long process, taking 10 to15 years, and failure rates are astonishingly high (only 7% of vaccine development projects reach preclinical development and licensure). Before COVID-19, the fastest vaccine developed was Merck & Co.’s mumps vaccine (part of MMR) which took four years to develop. Naturally, the speed of COVID-19 vaccine development was accompanied by skepticism. According to a 2021 poll by the American Psychiatric Association, 1 in 5 Americans said they would not be vaccinated for reasons that include the vaccine was developed too fast.
The COVID-19 vaccines are not as new as many might think. At first glance, it is true that the virus’s genetic sequence is novel, shared publicly by China on 12 January 2020. But, the technology to deliver the viral sequence already existed. In fact, many of the COVID-19 vaccines can be attributed to research conducted during the Ebola virus outbreak of 2014.
Ebola research began back in the 1970s and progressed in Canada’s federal National Microbiology Laboratory. However, the vaccine mainly sat on the shelf. Since Ebola is a rare disease, typically affecting a resource-poor part of the world, with low transmission rates (due to high mortality and low spread), pharmaceutical companies had no financial incentive to make a vaccine for Ebola per se. The outbreak of 2014-16, the largest in recorded history, posed a unique opportunity for Ebola technological development. Whether one views this period as a humanitarian feat or as a biosecurity defense mechanism, it was nonetheless an opportunity for companies to scientifically explore potential therapeutics in their pipelines. The 2014 outbreak resulted in several platforms using various vectors to deliver the virus, two of which are FDA approved: Everbo (Merck & Co. 2019) and Zabdeno®+Mvabea® (Janssen 2020).
A platform is a vaccine tool used as a delivery vector that can be recycled for many different target viruses. Platforms have been called “plug and play” because one can “plug in” the virus of interest onto the platform and “play” it in the human body. It is like having a school bus that drops off different kids throughout the day. The transportation remains the same, but the content inside is changed.
There is no immediate market for platforms (i.e., the Ebola market), but their value lies in future applicability. When Merck bought the Everbo vaccine from NewLink Genetics in 2014, the licensing agreement allowed Merck to have exclusive rights to the vaccine along with subsequent products. This means that Merck was able to keep the rights to the platform for any future application that could be of benefit to the company, thereby allowing market expansion into other diseases. In this way, companies can profit without producing. This reflects a theme of financialization whereby companies re-use existing assets in lieu of making new products, reducing development costs and maximizing revenue. In fact, in 2017, the World Health Organization (WHO) proposed a guideline for Ebola vaccines in which they stated that if robust data from prior use of the same platform against another viral antigen was available, both immunogenicity and toxicity studies could be skipped, and Phase I trials could begin. While the Ebola market may not have existed, there was potential to re-use platform technology for other diseases.
The incentive of profiting from Ebola platform recycling is proven by the COVID-19 vaccines. Figure 1 shows the companies and vectors involved in Ebola vaccines, COVID-19 vaccines, and the platforms which have been recycled.
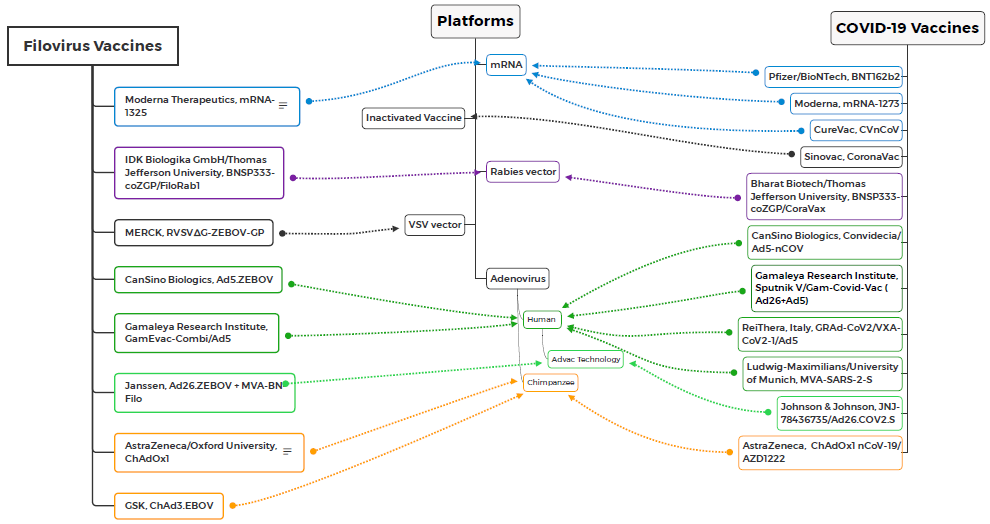
Merck used the same VSV platform used for the Everebo vaccine to create the COVID-19 vaccine candidate V590. However, adenovirus platforms (Ad) are the most common viral vector, including types Ad5, Ad26, and Modified Vaccinia virus Ankara (MVA). Janssen created a two-dose preventative Ebola vaccine regimen involving a first dose of Ad26.ZEBOV (Zabdeno), and a second dose of MVA-BN-Filo (Mvabea) eight weeks later. Zabdeno is based on Janssen’s AdVac® viral vector technology and served as the template vector for Janssen’s Ad26CoV2-S COVID-19 vaccine, also known as ENSEMBLE (JNJ-78436735).
The most frequently used Ad vector is Ad5. The Gamaleya Research Institute developed the Ebola vaccine GamEvac-Combi/Ad5 involving two doses: one priming immunization of VSV and a booster of Ad5 three weeks later. Gamaleya used this approach in developing Sputnik V/Gam-Covid-Vac, which also involves a two-dose regiment of Ad26 and Ad5. CanSino Biologics also developed an Ad5-based Ebola vaccine, Ad5-EBOV, composed of human Ad5 expressing Zaire Ebola virus (Makona isolate) with an envelope glycoprotein. Phase III trials were never conducted because the Ebola epidemic ended in 2016. Regardless, in 2017 the China Food and Drug Administration approved the Ad5-EBOV vaccine, and CanSino used the same vector to make their Convidecia/Ad5-nCOV COVID-19 vaccine.
To avoid pre-existing anti-human adenovirus immunity, the University of Oxford developed a chimpanzee Ad-vector, ChAdOx1. ChAdOx1 was first used in combination with the MVA poxvirus vector against influenza (MVA/ChAdOx1). Other studies have shown the vaccine’s effectiveness in Rift Valley Virus (RVF) and Crimean Congo Haemorrhagic Fever virus, among others. The data collected in previous clinical studies were used to accelerate COVID-19 vaccine development. The University of Oxford licensed AZD1222 to AstraZeneca, which produced the ChAdOx1 nCoV-19/AZD1222 COVID-19 vaccine.
The only vaccine platforms that did not end up as a COVID-19 vaccine were SinoVac, an inactivated virus, and GlaxoSmithKleine’s ChAd3.EBOV vaccine. The Moderna and Pfizer/BioNTech mRNA platforms were used predominantly in cancer research but had also been tested for Zika virus using mRNA-1325. Merck tried to build on the Ebola vaccine’s success by making a VSV-based COVID-19 vaccine, but the results were not good enough compared with the other COVID-19 vaccines on the market.
The rapid creation of COVID-19 vaccines stunned the world, and the accelerated development can be attributed to work done years prior during the Ebola outbreak in 2014. The vaccines were not spontaneous inventions but tools that leveraged existing resources and repurposed them for the pandemic. The speed of COVID-19 vaccine development is like receiving a package from Amazon: whether you get prime same-day delivery or regular shipping, the quality of the content inside is the same. The years of research that went into Ebola platform technology can explain the speed of COVID-19 vaccine development by reusing existing vectors for new therapeutic applications.

Pingback: Decolonizing Global Health: The opportunities and pitfalls presented by reform of the Health Emergency Preparedness, Response, and Resilience (HEPR) Architecture – The Graduate Press